

Revision rhinoplasty
Aesthetic and reconstructive nose surgery
What is revision or secondary rhinoplasty?
Revision rhinoplasty is a surgical technique that modifies the nose of a person who has already undergone rhinoplasty.
It can be offered to correct unsatisfactory results of rhinoplasty.
It can also be used to improve already satisfactory results. It affects 9 to 10% of patients undergoing a first rhinoplasty. (reference: Neaman et al., Aesthetic Surgery Journal, 2013).
Here we will discuss the different aspects of secondary rhinoplasty, including the reasons why it is performed, the different techniques used, the risks and the possible benefits, as well as the information necessary to prepare for the operation.
Why do revision rhinoplasty?
In the event of a functional problem
The nasal obstruction may be linked to a deviated septum which was not treated during the first operation, or which was revealed following a reduction in the size of the nose.
In this case it is entirely possible to repair the septum in order to keep it straight.
On the contrary, a first rhinoplasty is generally not responsible for disorders of the nose.
sense of smell.
Some patients report a feeling of runny nose which seems to have appeared following the first operation. This is common yet the explanations are not clear as the mucous membrane has not been modified.
In rare instances, it is possible to feel pain, particularly when wearing glasses, due to excessive thinning of the “soft parts” that ensure the interface between the skin and a nasal structure isn’t too protruding. This is treated by rasping the structure and reestablishing the missing interface using a graft.
In the case of aesthetic problems
Examples most frequently encountered in revision rhinoplasty
Residual nose deviation
The deviations are treated by straightening the wall of bone and cartilage, primarily with the use of an ultrasonic rhino-sculpture tool. Noses that have a residual deviation frequently have a high septal deviation that will need to be corrected.

Dorsal scar
In these cases, it is not possible to make the scar disappear without creating others, although a “lipostructure” fat graft can improve it.
Furthermore, reducing the size of the nose makes the scar less obvious.

Nasal bones too wide
In these cases, it is necessary to sculpt the wall of bone and cartilage to reduce the width.
Furthermore, it is possible to reduce excess bone by “rhinoscuplting” with ultrasonic device or with a rotary burr.

Nasal bones too pinched
In these cases, two alternatives are possible: it is possible to cut the bony structure "osteotomies", spread the bones and then insert a spreader (generally with a cartilage graft). The other alternative, simpler yet just as effective, is to inject chopped cartilage into the sunken areas.

Inverted V
The inverted V is the most classic postrhinoplasty sign, allowing you to immediately recognize a patient who has already had surgery. It can appear 6 to 9 months after a first rhinoplasty.
The inverted V corresponds to a collapse in the cartilages of the back of the nose, appearing in rhinoplasties with significant dorsal reduction without strengthening of the middle third of the nose.
This aspect is treated by the placements of cartilaginous grafts, the “spreader grafts”.

Polly beak deformity
The so-called “polly beak deformity” appearance corresponds to a curve seen in profile between the tip and the back of the nose.
This appearance is generally due to the combination of two factors : insufficient removal of the nasal septum (this is why the pollybeak is hard in palpatione and moves with the septum) and a collapse of the tip due to structural insufficiency.
This is treated by reduction of the excess septum and reinforcement of the tip.
More rarely, pollybeak is due to an accumulation of fibrosis. In this more delicate case, fibrosis can be reduced during surgical revision.
Nasal saddling
Nasal saddling is the appearance observed when the nasal septum has collapsed and takes away the lower part of the dorsum. This is the opposite of polly beak. and is frequently associated with respiratory disorders.
This aspect is treated by reconstructing the nasal septum, most often with a costal cartilage graft.
Harmonious but too big nose
In these situations, the first rhinoplasty was performed well but the nose was still considered too large by the patient. This is a very delicate situation because the benefit / risk balance is not necessarily in favour of a new intervention.

Nasal dorsum cyst
In this situation, we notice a soft pocket on the back of the nose, varying in volume depending on the day.
This complication, rare but classic, is linked to the installation of a graft containing a small fragment of mucosa, which will systematically transform into a cyst.
This cyst must be completely removed during surgical revision.

Excessive resection of the tip cartilages
The cartilages of the tip are frequently reduced during a first rhinoplasty. If this is done excessively, especially on weak cartilage, it can lead to drooping of the tip, as well as retraction of the wings of the nose.
This condition is treated by reconstruction and / or strengthening of the cartilage, using cartilage grafts.
This is a particularly difficult technique which should only be carried out by a trained surgeon.

Malposition of the tip cartilages
The cartilages of the tip are frequently worked and modified by sutures during a first rhinoplasty.
If this is done inappropriately, it can lead to malposition of the tip, as in the attached photo .
In this case, it is necessary to undo the sutures, reinforce the cartilages with grafts and replace the tip in the correct position.
This is a particularly difficult technique which should only be carried out by a trained surgeon.
Deterioration of subcutaneous tissues
This aspect is observed after several rhinoplasties, particularly if there has been very extensive subcutaneous degreasing.
In these particularly complex situations, it is possible to offer fat injections (lipostructure) and sometimes hyperbaric chamber sessions.
In certain cases, the benefit / risk balance does not allow us to consider new intervention.

Complications after implant placement
Silicone, Medpore or Gortex implants are often offered to recreate a nasal bridge.
These implants lead to frequent complications such as infection and rejection causing unsightly scars at the tip. Revision surgery is subsequently very difficult.
The ideal is to remove the implant before it becomes infected and replace it with a cartilage graft.
Technique used to correct rhinoplasty:
Cartilage grafts
Depending on the cases, it may be necessary to take cartilage grafts from the ears or ribs, although they are generally taken from the nasal septum (the septum). As part of a secondary rhinoplasty, it is common for the septum to be lacking, so it may be necessary to take cartilage from the ears (the concha) or the ribs.
The concha is the cartilage located behind the ear. Taking it does not change the shape of the ear if it is done according to the rules of art. It is a graft that is easy to harvest and causes little pain.
Its disadvantage is its thickness and lack of rigidity, which makes it of little use for advanced reconstruction.
Rib cartilage is the graft of choice in multi-operated patients.
It is customary to take one or two rib fragments by making a small incision under the chest on the right.
This results in a scar which is usually very discreet. The pain is moderate for 10 days.
Rib cartilage makes it possible to obtain a large quantity of very good quality grafts. Its main disadvantage is that it can twist slightly over time.
The objective is to restore a functional and aesthetic anatomy, which is stable over time.
Am I a good candidate for surgery?
The best candidates for secondary rhinoplasty are those who are in good emotional and physical health, as well as realistic about the potential improvement. A person with a secondary nasal problem should strive for improvement, not perfection.
Depending on the type of deformity, nasal shape or function may or may not be completely improved..
Deciding to have secondary nasal surgery should not be an impulsive decision, but rather a carefully considered decision.
That's why it's important to be realistic, to be informed and to be true to yourself about what really bothers you about the outcome.
How long does the procedure last?
A secondary rhinoplasty takes place under general anesthesia and lasts between 2.5 and 6 hours for the most difficult procedures.
Get more information by following these links
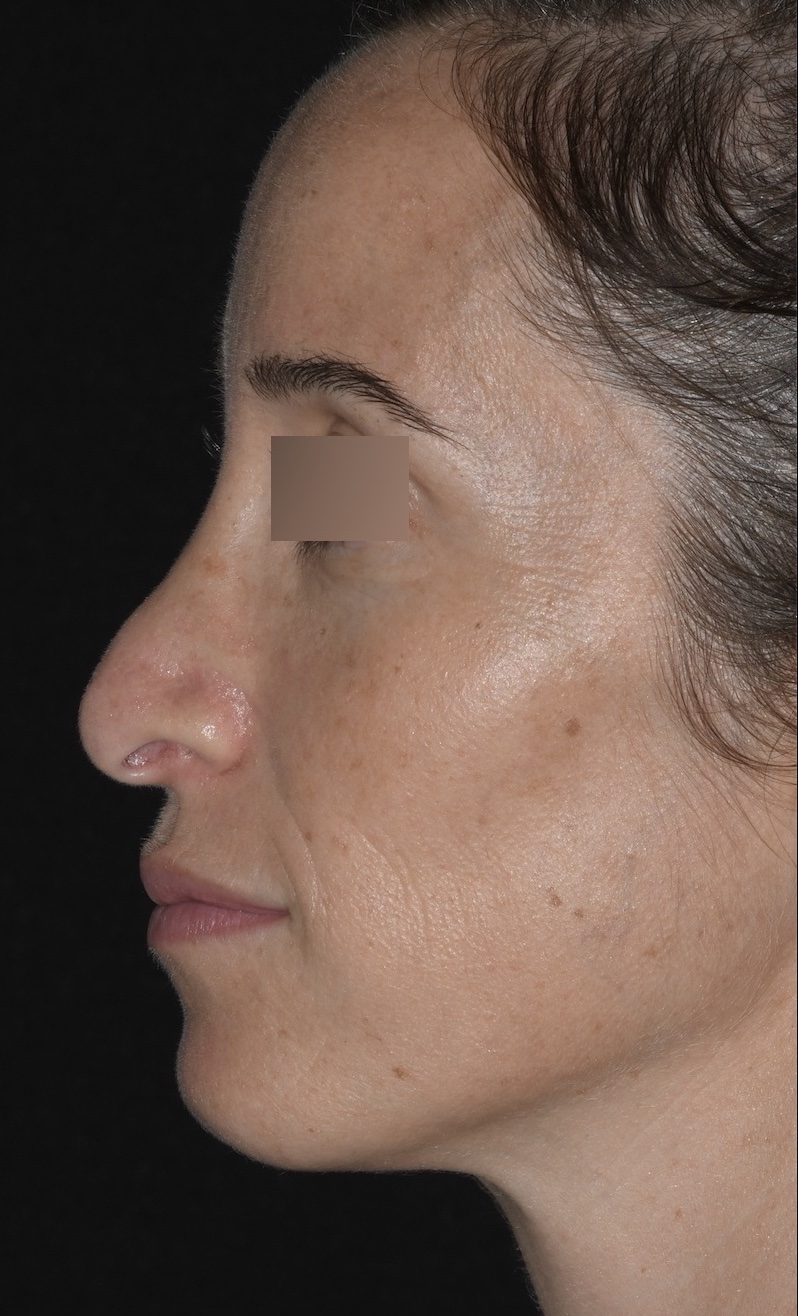
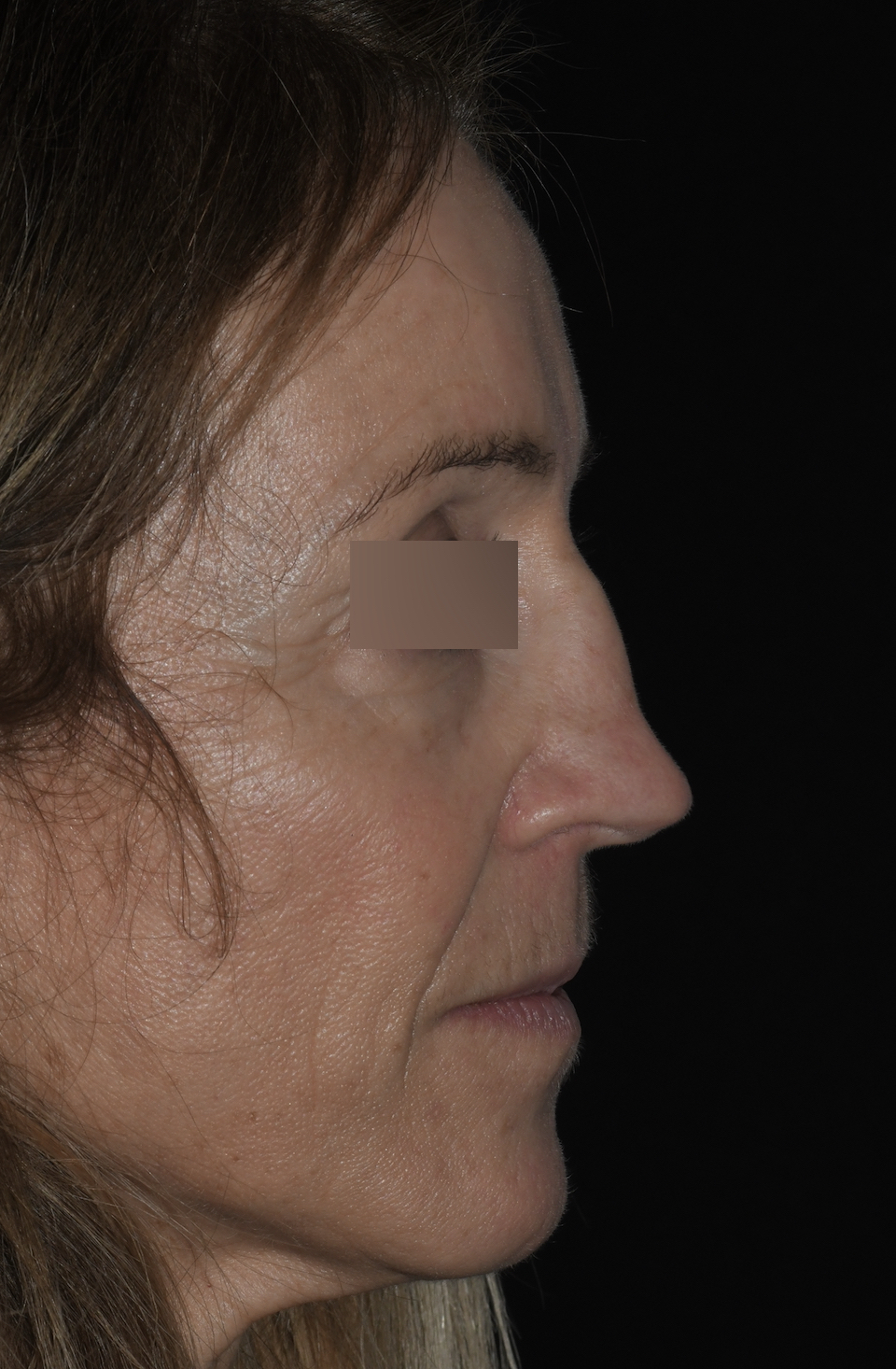
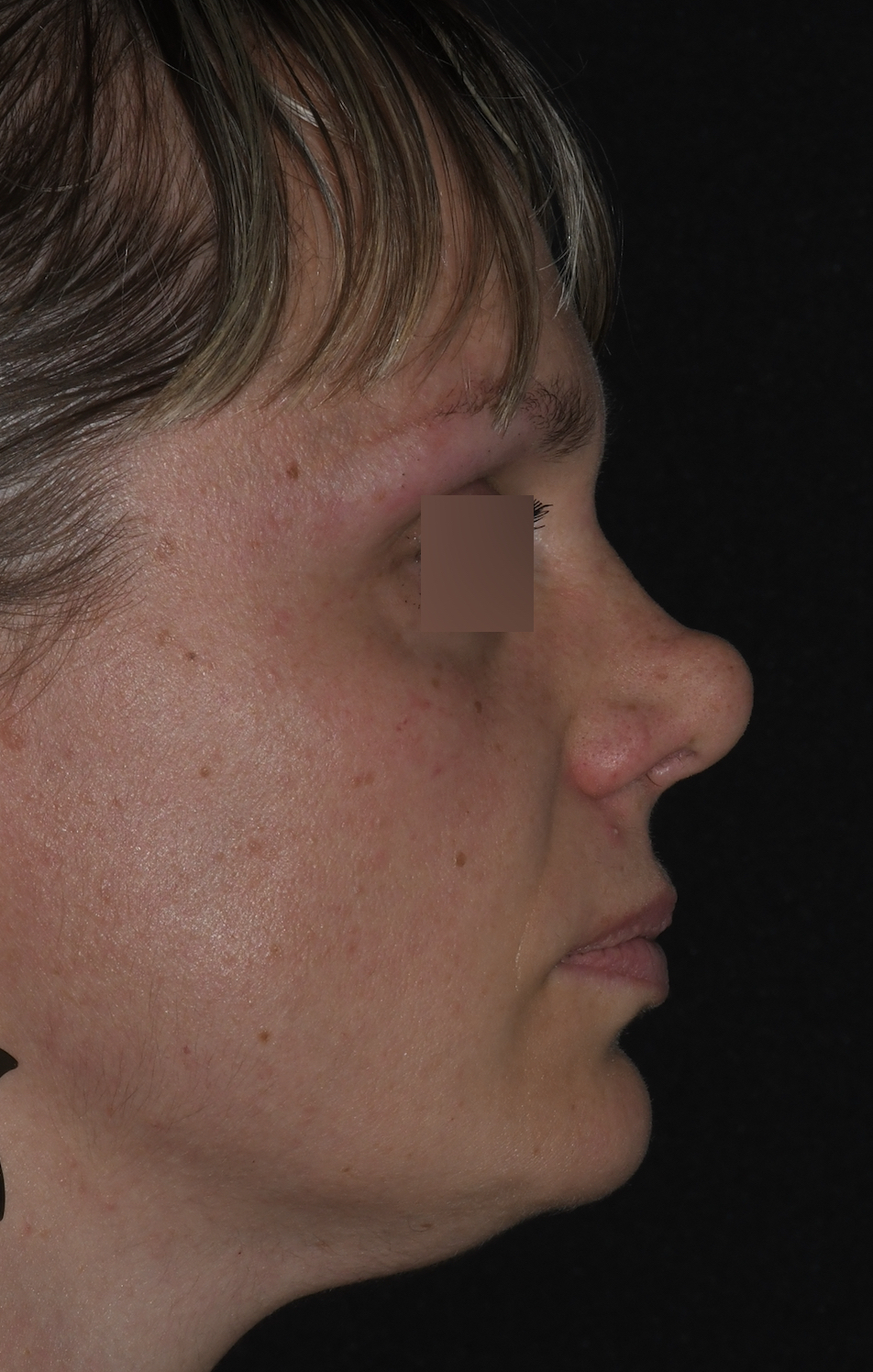
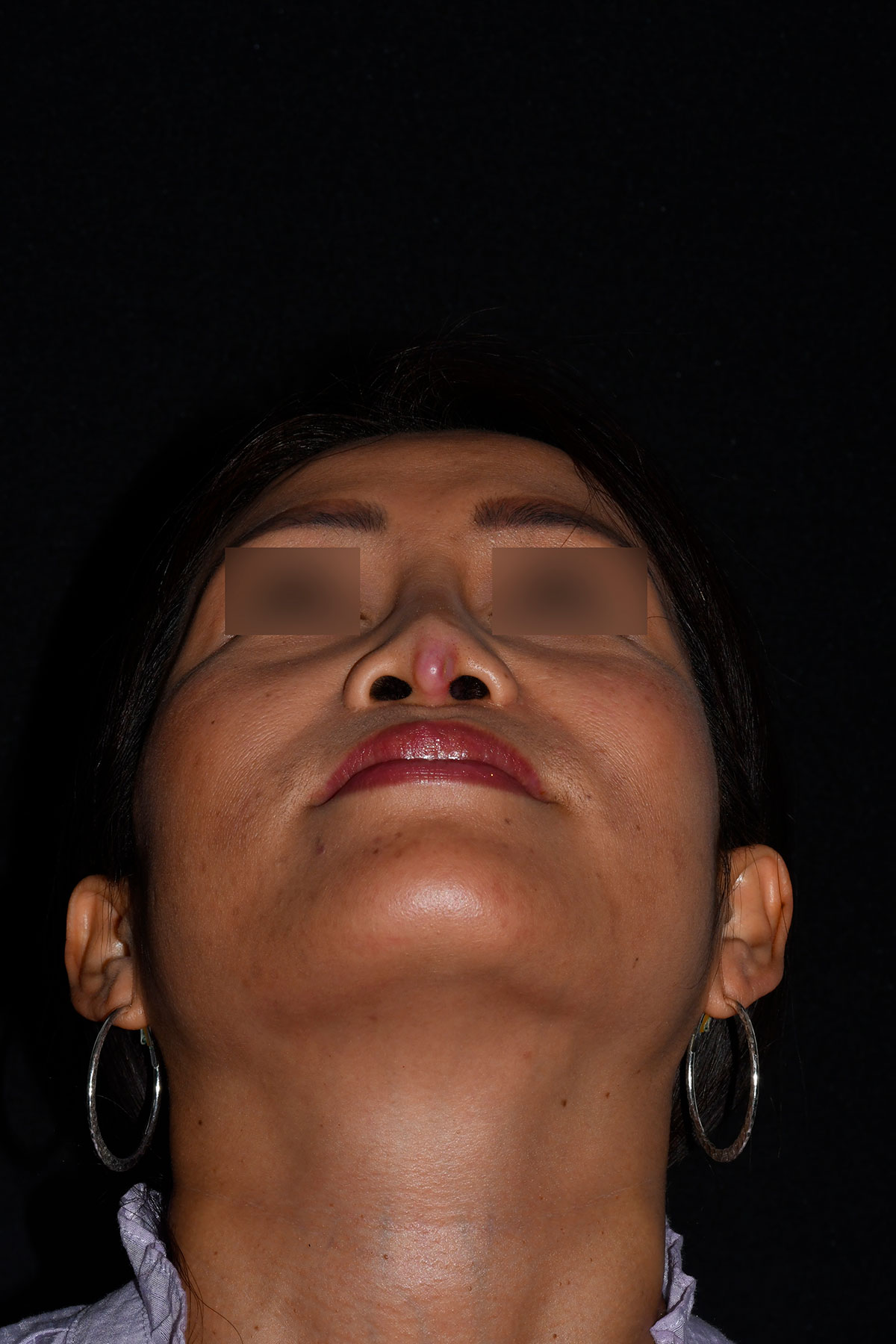
The attached photos have been published with the kind consent of the patients in order to illustrate the different situations.
Their reproduction and use is strictly prohibited.